大腿内側の痛み
みなさん、こんにちは。
先日の指導で迷った症例。
専攻医のコンサルトはこんな感じ↓
28歳女性、最近太ってきて70kgくらいある。
数週前から片側大腿内側にビリっとする痛みが1日2回くらい出る。
誘発因子なし、痛みは一時的、もしかしたら反対側も出てきた?
随伴症状なし。
貧血の指摘はあり鉄剤飲んでいる。
神経痛かな〜と思うのですが、どうしましょう?
大腿の外側なら、外側大腿皮神経の絞扼性障害を思い浮かべますが、内側では…?
神経痛とすると、まずは分布の確認です。
いつもこんがらがるのですが、以下の違いを認識しておくことが必要です。
・デルマトーム:一つの脊髄分節〜神経根が支配する領域
・皮神経:複数の脊髄分節から出る繊維が集合した神経が支配する領域
(ミオトーム、スクレロトームなんてのもあるらしいです。リンク先参照)
「一般に、上肢ではデルマトームに重なりや個人差が多いためミオトームの信頼性の方が高く、下肢ではその逆とされている」と書いてある文献もありました。
https://www.jstage.jst.go.jp/article/jscn/41/3/41_151/_pdf/-char/ja
ネットで拾った資料をまとめてみます。
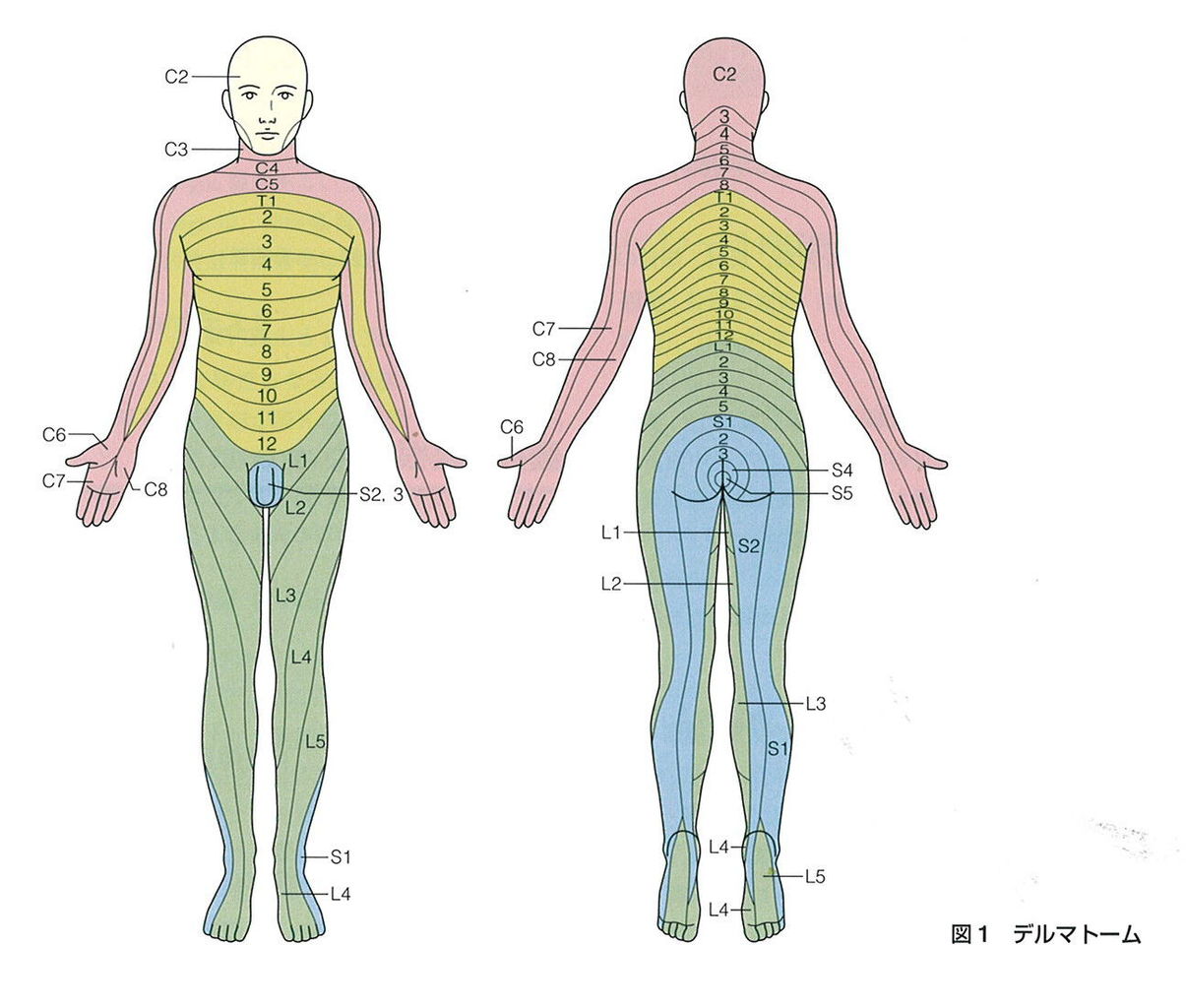
まずはデルマトーム。
・イラスト解剖学でしょうか。ランドマークがわかりやすいですね。
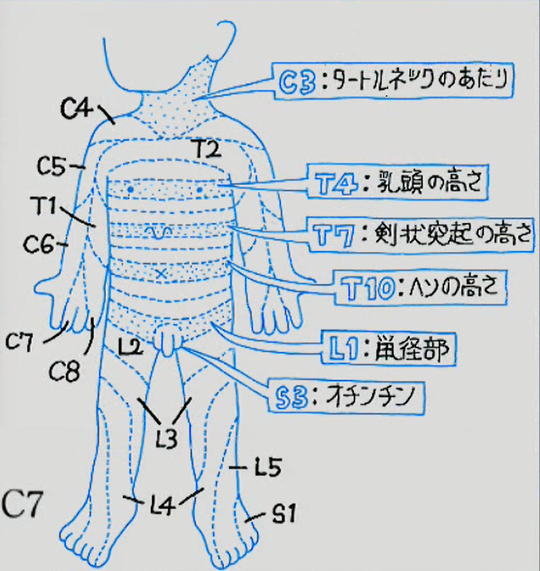
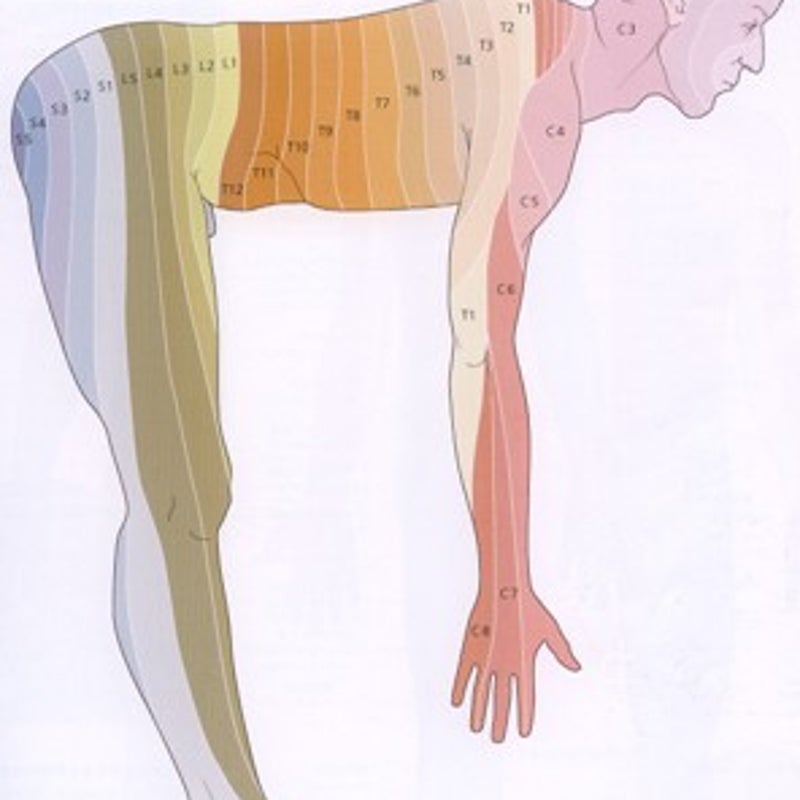
・人間ってもともと4本足だったんだな〜ということを再認識する図。
・感染症の先生のブログより。
続いて皮神経。
・接骨戦士のブログより。

(追記)
下肢の感覚に関わる神経系は以下の通り(参照:イラスト解剖学第6版)
腰神経叢→陰部大腿神経(L1, L2)
→ 外側大腿皮神経(L2, L3)
→大腿神経(L2-4)→前皮枝(L2, L3)
→伏在神経(L3, L4):内転筋管で圧迫されることがある
→閉鎖神経(L2-4)
仙骨神経叢→後大腿皮神経(S1-3)
→坐骨神経(L4-S3)→総腓骨神経(L4-S2)→外側腓腹皮神経(L4-S1)
→浅腓骨神経(L4-S1)
→深腓骨神経(L4-S1)
→脛骨神経(L4-S3)→腓腹神経(S1, S2)→外側・内側足底神経
腰神経叢は「後面を除く大腿と下腿の内側面」に
仙骨神経叢は「大腿後面と下腿〜足」に分布する。
改めて、解剖学の本は大事ですね。
ちなみに坐骨神経痛に関する大浦先生のブログはこちら↓
今回だと、閉鎖神経や大腿神経前皮枝あたりかと思います。
もしくはL2-4あたりの神経根も考えられますが、それだと更に足先に向かっての症状もあってほしいところですね。(神経根症と鼠径部痛についての研究)
そして、支配神経にあたりをつけたら、次にどこで障害が起こっているかを考えます。そのためには解剖のおさらいが必要です。
閉鎖神経(Obturator nerve)の走行はこちら。

UpToDate:Overview of lower extremity peripheral nerve syndromesを参照すると
閉鎖神経麻痺
Mononeuropathies of the obturator nerve are uncommon. They present with pain, weakness in leg adduction(内転), and sensory loss over a small area in the medial thigh. There is no compelling evidence of a true obturator entrapment neuropathy caused by a narrow obturator foramen [23]. However, obturator neuropathy does occur secondary to pelvic trauma or surgery. In addition, one study suggested that isolated obturator neuropathy can be the sole manifestation of pelvic cancer, most commonly transitional cell carcinoma of the bladder [24]. (See "Nerve injury associated with pelvic surgery", section on 'Obturator nerve'.)
二次性に起こる(骨盤外傷や手術、膀胱癌などの骨盤内腫瘍による)ことはあるけれど、いきなり単独で絞扼症状がでるかというとはっきりしていないようです。
鍼灸師やリハビリ?のサイトにはしばしば麻痺が起こるということが書いてあります。
閉鎖孔を通るところでの障害が多いようで、内閉鎖筋・外閉鎖筋・大腰筋によって影響を受けるようです。また、閉鎖孔ヘルニアで起こることもあります(Howship-Romberg sign:こちらのサイトも参照)。
下肢の内転に携わる筋肉も支配しているので、筋力低下がないかも調べなければなりませんね。
(追記)
閉鎖神経は骨盤壁内面の壁側腹膜にも感覚枝を出しているため、骨盤臓器の炎症などでそこが刺激を受けたときに、大腿内側に関連痛が出る事がある。
大腿神経(Femoral nerve)の走行はこちら。

こちらのサイトも参考になります。
UpToDate:Overview of lower extremity peripheral nerve syndromesを参照すると
大腿神経麻痺
Compression of the femoral nerve is relatively uncommon due to its position within the pelvis and anterior thigh. Nevertheless, hip or pelvic fractures or masses within the iliacus (such as hematoma) can sometimes result in a femoral neuropathy. The true incidence of iatrogenic femoral nerve injury is unknown, but the syndrome is a recognized complication of childbirth and procedures such as hip replacement, abdominal and pelvic surgery or laparoscopy, inguinal lymph node biopsy, femoral nerve block, and femoral artery puncture [17-19]. One report suggested that femoral neuropathy was caused by prolonged maintenance of the lithotomy position itself with compression of the inguinal ligament upon the nerve, rather than a specific surgical procedure [20]. In addition to compression, other potential mechanisms of iatrogenic femoral nerve injury include transection, diathermy, toxic injury, and ischemia [18,19].
Patients with diabetes mellitus occasionally develop spontaneous femoral neuropathies. However, it is debated whether this simply represents a more limited form of diabetic amyotrophy (see 'Diabetic amyotrophy and idiopathic lumbosacral radiculoplexus neuropathy' below). The mechanism of this is presumably nerve infarction.
On examination, patients with significant femoral neuropathies develop weakness involving the quadriceps muscle group with sparing of adduction, which is mediated by the obturator nerve. One argued point is whether or not the iliopsoas is innervated by the femoral nerve or a direct branch of the plexus; regardless of the strict answer, it is clear that some patients with what appear to be isolated femoral neuropathies also have prominent iliopsoas weakness. In addition to muscle weakness, sensory loss over the anterior thigh and most of the medial thigh is typical. The sensory loss extends down the medial shin to the region of the arch of the foot due to saphenous nerve dysfunction. The knee jerk generally decreases or becomes unobtainable.
鼠径部での絞扼は起こりうるようですが、腸腰筋の筋力低下も起こるはず。
前皮枝単独での障害について書いてある記事は見つけることができませんでした。
ということで、この方はとりあえず腰部神経根に異常がないことを確認し、症状フォローとしました。次来られたときには筋力低下も確認しないとですね。
ちなみに閉鎖神経ブロックという手技もあるようです。
経尿道的手術の下肢内転予防の他、膝・股関節の鎮痛補助に使われます。
まとまっている資料はこちら。
http://www.ntmc.go.jp/ntmc/uploads/fckeditor/sinryo/Masuika/uid000015_SPP-25_2015032481c5c8ec.pdf